
The definitions of a “case” and “hospitalization” were dramatically loosened for this pandemic
NBC reported a serious uptick in U.S. Covid-19 hospitalizations in mid-November. However, when we examine the data provided we see that the “meat” of the story, beyond an unfortunate uptick in hospitalizations and deaths in El Paso, Texas, is the Covid Tracking Project’s data on increased numbers of Covid-19 hospitalizations.
But a “hospitalization” is defined as someone in the hospital who has tested positive for Covid-19 at some point previously — not necessarily in the hospital because of the virus. This is an extremely broad definition that ignores normal rules of causality required for diagnosis and medical data tracking.
The rest of this essay will look in detail at the new definitions of “case” and “hospitalization” and attempt to explain how these key definitions were dramatically loosened in 2020. I also explain how these definitions form the beginning of the pandemic tracking chain and how these loosened definitions have affected the pandemic.
Quick summary: overly-inclusive definitions of “case” and “hospitalization,” combined with often wildly inaccurate Covid-19 tests, and dramatically increased testing, have together resulted in significant inflation of the perception of the pandemic’s severity as we head into the winter.
The following figure shows why these definitions are important. My next essay will flesh out the various parts of this figure.

How is a “case” defined?
My copy of the Gordis Epidemiology textbook has this to say about the definition of a “case”:
The CDC defines the surveillance case definition as “a set of uniform criteria used to define a disease for public health,” which is intended to aid public health officials in recording and reporting cases. This is different from a clinical definition that is used by clinicians to make a clinical diagnosis to initiate treatment and meet individual patients’ needs.
However, the CDC dramatically loosened the definition of “case” in an April 2020 Covid-19 guidance document, which provided that a confirmed “case” could rely solely on a positive test. There was no requirement that any symptoms be identified. Historically, a “case” of a specific disease required symptoms as well as lab testing. The new definition also has a very loose set of clinical criteria (symptoms) that can be relied on for identifying cases.
The new CDC Covid-19 case definition (updated August 2020), recommended first by the Council of State and Territorial Epidemiologists (CSTE), has four different categories for identifying a Covid-19 case:
- Clinical criteria
- Laboratory criteria
- Epidemiologic linkage
- Vital records criteria
The “clinical criteria” for identifying a case are incredibly inclusive when compared to other historical outbreaks such as the SARS and MERS case definitions (the two previous novel coronavirus respiratory syndrome outbreaks in the last twenty years). For example, the CDC guidance provides that any one of the following symptoms, in the absence of a more likely diagnosis, is enough to conclude a person, combined with epidemiological data (which I describe below), is a “probable case” of Covid-19:
- cough,
- shortness of breath,
- difficulty breathing,
- new olfactory disorder,
- new taste disorder (these last two were added in the August update to the case definition)
The epidemiological criteria are also very inclusive, as follows:
- Close contact with a confirmed or probable case of COVID-19 disease;
- Member of a risk cohort as defined by public health authorities during an outbreak.
There is a second list of potential symptoms and the CDC guidance provides that at least two of the following symptoms, when combined with epidemiological criteria, are sufficient to conclude that a person has Covid-19:
- fever (measured or subjective),
- chills,
- rigors,
- myalgia,
- headache,
- sore throat,
- nausea or vomiting,
- diarrhea,
- fatigue,
- congestion or runny nose
So a simple cough and contact with someone who tested positive for Covid-19, is enough, based on this official guidance, to conclude a patient has Covid-19, regardless of the fact that there are numerous other viruses and bacteria that cause coughing, including the well-known family of common cold coronaviruses (CCC), of course.
Or a headache and a sore throat and contact with someone who tested positive for the virus is enough to diagnose that person as having Covid-19.
But no symptoms at all are required for a “confirmed case” under the “laboratory criteria” category. It is enough under this category that a patient have a positive PCR test or an antigen test.
However, both of these tests can be wildly inaccurate, with 90% or more effective false positives (either inherently or in how these tests are being used) or false negatives in many circumstances, for both kinds of tests. My previous essay examined the accuracy of these tests in detail. It is hard to over-state the importance of these two items (i.e., a very loose case definition and often wildly inaccurate Covid-19 tests relied on for identifying cases) in understanding the nature of the pandemic.
There is a third category of clinical criteria that are perhaps even more broad than the first two lists discussed above:
— Severe respiratory illness with at least one of the following:
- Clinical or radiographic evidence of pneumonia,
- Acute respiratory distress syndrome (ARDS).
Again, these clinical criteria combined with the very weak epidemiological linkage is enough to conclude the patient has Covid-19, despite the fact that pneumonia has been extremely common for hundreds of years before the novel coronavirus was discovered.
The CDC provides a page on the history of the surveillance case definitions for various diseases. Uniform case definitions for a number of diseases were first established by CDC and CSTE in 1990. The last time the criteria were modified was in 1997. The 1997 report states:
“These case definitions are to be used for identifying and classifying cases, both of which are often done retrospectively, for national reporting purposes. They should not be used as criteria for public health action.”
This admonition has clearly not been heeded with respect to the coronavirus pandemic.
Recent case definitions from CDC on, for example, the SARS outbreak in 2003 and the H1N1 in 2008, required clinical symptoms plus laboratory confirmation for a case to be “confirmed”. The CDC’s 2003 case definition for SARS requires (p. 2): “Clinically compatible illness (i.e., early, mild-to-moderate, or severe) that is laboratory confirmed.”
The influenza (flu) case definition, last updated in 2012, also requires both clinical and lab evidence for a confirmed case: “A case that meets the clinical and laboratory evidence criteria.” The CDC’s “confirmed case” definition for Covid-19 requires only “confirmatory laboratory evidence.”
So the 2020 case definition for Covid-19 was in key ways a substantial break from the policies in place for decades prior to 2020. This change in case definition alone played a major role in transforming what might otherwise have been akin to a significant flu/pneumonia/cold season into a major global pandemic. (I will examine the excess deaths count in detail in a later essay).
In sum, the new CDC Covid-19 surveillance case definition adopted a very loose set of criteria when it was adopted in April of 2020, setting up the U.S. for a self-reinforcing chain of pandemic data that rests largely on this new case definition and a number of laboratory tests that are in many cases wildly inaccurate.
Both the mainstream media and our public health professionals are failing to recognize the key distinctions between surveillance case definitions and clinical criteria for identifying confirmed cases of Covid-19. The end result is an extremely loose surveillance case definition being used in making public health policy — expressly against the guidance that the CDC itself has historically provided.
We’ll look next at how “hospitalizations” are defined.
How is a “hospitalization” defined?
CDC defines a Covid-19 “hospitalization,” for purposes of surveillance, as any patient hospitalized within 14 days of a laboratory-confirmed positive coronavirus test that was ordered by a healthcare professional.
The CDC’s COVID-NET is a “surveillance system that collects data on laboratory-confirmed COVID-19-associated hospitalizations.” CDC also states on the same web page: “COVID-NET is CDC’s source for important data on hospitalization rates associated with COVID-19.” And: “Cases are identified in COVID-NET if they test positive for SARS-COV-2 (the virus that causes COVID-19 disease) through a test ordered by a health care professional and are hospitalized within 14 days of the positive test.”
However, in practice, most states are reporting Covid-19 hospitalizations as anyone who has tested positive at any point, with any kind of test, and at any point in time, not just within 14 days of the hospitalization. Needless to say, this is far looser than the relatively cautious definition adopted by COVID-NET.
For example, the Covid Tracking Project created by The Atlantic magazine (widely used to track nationwide hospitalizations rather than the more stringent CDC data) definition of hospitalization reflects this much looser definition of a hospitalization (click on the “expand all” link below “definitions” on the left side of the page), as follows:
“Individuals who are currently hospitalized with COVID-19. Definitions vary by state / territory. Where possible, we report hospitalizations with confirmed or probable COVID-19 cases per the expanded CSTE case definition of April 5th, 2020 approved by the CDC.”
I discussed above how expansive (“expanded” as the above quote states) the new definition of “case” is. And when the widely reported Covid Tracking Project data is based on this definition, including not only confirmed cases but also probable cases, occurring at any point in time before hospitalization, it’s easy to see how the huge increase in reported hospitalization figures in the U.S. is a result of these loosened definitions. The NBC story at the beginning of this article relies on the Covid Tracking Project hospitalization figures.
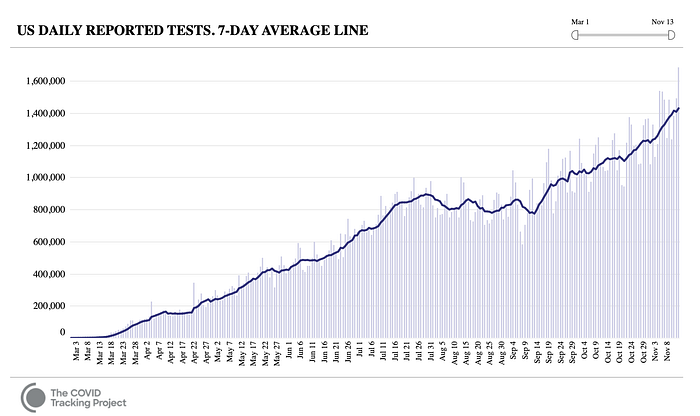
It’s also the case that testing in the U.S. in general has dramatically increased — often commensurate with the increase in reported cases. As this chart shows, testing has more than doubled (from as low as 582,000 tests Sept. 8 to almost 1.7 million on Nov. 13, the last day in the chart) in almost exactly the same timeframe that cases have doubled. A state-by-state analysis shows that most states mirror this aggregated nationwide trend in seeing a good correlation between increased testing and increased cases and hospitalizations.
Positivity rates (this is the percent of tests that come back positive) have also doubled in roughly the same time frame, however, and this would be cause for some concern if the various coronavirus tests weren’t wildly inaccurate, either inherently or in how they’re being used, as my previous essay described.
In closing, as a policy lawyer with almost 20 years of experience I strongly urge public health policymakers and medical professionals to look closely at this chain of definitions and diagnostic and surveillance tests, and consider how these various policy choices are affecting our collective understanding of the pandemic — and what public policy choices should be made in light of a revised understanding.
