Biden’s promise of massive increases in home-based rapid antigen tests is exactly the opposite direction we should be going because of the inevitable tsunami of false positive results that come from widespread testing of asymptomatic people with flawed tests; we are already well into “casedemic” territory now and Biden’s new approach will extend our casedemic for an indefinite period, until we understand better how increased asymptomatic testing leads to huge numbers of false positives
President Biden, in a new approach to the pandemic announced the week before Christmas, promised five hundred million free COVID tests for the American people. The idea is to allow people to test themselves before attending social events, school, going to work, etc., and to know, almost in real time, whether they may be infectious.
On its face, this seems like a very reasonable approach. Why wouldn’t having more information about possible infections be a good thing?
But it’s actually a really bad idea. Mass testing of people who are overwhelmingly asymptomatic (showing no symptoms) will in fact inevitably extend this pandemic nightmare for additional months and maybe even years as “cases” continue to mount from false positives. To be clear: Biden’s mass testing approach is exactly the opposite of what is needed right now. We should not be testing asymptomatic people at all.
We can do the math, using well-established principles of epidemiology. With 500 million rapid tests deployed for free by the Biden administration, and used to test people who are asymptomatic (which will be the case in the vast majority of circumstances in schools, social events, universities, workplaces, when traveling, etc.), and a generous assumption of 1% background disease prevalence (it’s been far lower than this during most of the pandemic in the U.S., as discussed in this essay) and 98% specificity (antigen tests can be far lower accuracy than this, particularly for at-home test use), we will have about 9.9 million false positives resulting from these tests. That’s a tsunami of false positives.
Let’s examine the math a little deeper. The following chart is from the BMJ online rapid antigen test (what they call “lateral flow tests,” using the British name for these tests) calculator. It shows 1,980 false positives for every 670 true positives, or a 75% false positive rate. This is the very definition of a “casedemic,” which is what happens when most cases are false positives or involve only mild symptoms.

If we use more realistic assumptions of 0.5% disease prevalence and 90% antigen test specificity, we get a catastrophic 97% false positive rate, with 9,950 false positives for every 335 true positives (see below figure).

We (Dr. Blaine Williams, Dr. Daniel Howard, and I) wrote a short essay for BMJ, which appears as a “rapid response” to the BMJ online calculator, that explains the scholarship demonstrating why testing asymptomatic people leads to massive numbers of false positives.
I’ve offered my policy prescriptions to end the pandemic in this essay here, where I discuss the need to change the Covid-19 “case definition,” eliminate testing of asymptomatics, and lowering the cycle threshold for PCR tests, but the rest of this essay will focus on why Biden’s approach to further increasing mass testing is the wrong way to go.
What is a case?
What defines a Covid-19 “case”? I’ve written many times previously about how unusual (almost unique) it was for the US CDC to define a “case” as a positive test result only. In the US the vast majority of cases are identified and tallied based only on a PCR or a rapid antigen test result only — no consideration of symptoms is required.
But this approach can lead to very large numbers of false positives being misidentified as “cases.” I’ve described this in previous essays as the “false positive paradox” or the “false positive catastrophe.” When this trend goes too far we find ourselves in a “casedemic” rather than a pandemic.
To get out of a never-ending casedemic scenario, which is where we’re clearly headed, we need to be very careful with our definitions, our testing procedures, and our data tracking.
Singapore tracks symptoms and severity of all Covid-19 cases and as of data available through end of December fully 99% of all their “cases” were asymptomatic or mild.
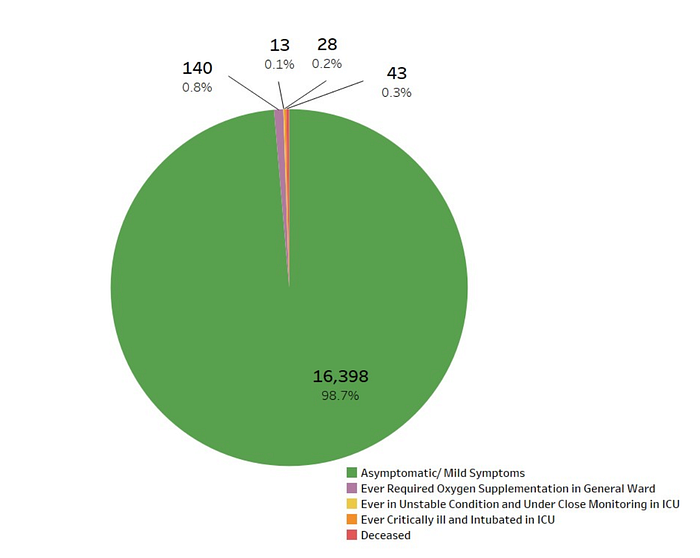
As a result of this overwhelming number of asymptomatic and mild cases, Singapore now focuses on hospitalization rates for tracking severity of the pandemic, and in making pandemic policy choices.
We don’t, unfortunately, track asymptomatic/symptomatic distinctions in our public data here in the US. We’re still very much focused on “cases” of any sort, no matter how mild or asymptomatic. Dr. Monica Gandhi at UCSF Medical School has warned about this trend and urged the US to adopt the Singapore approach by focusing on hospitalization figures rather than “cases”:
Learning to live with the virus in the long term will require changes in both mind-set and policy. Relying on Covid-19 hospitalizations as the most important metric to track closely will provide the most reliable picture of how an area is faring with the virus. And by focusing attention on the number of hospitalizations, health professionals can better focus on reducing them. This becomes especially important as case counts become more complicated.
Given our focus on “cases,” we have in recent days reached even higher heights of Orwellian absurdity with respect to tracking and responding to the virus. A recent Yahoo News article had the rather startling title: “What’s the difference between Omicron symptoms and cold symptoms? We asked an expert.” The answer from the expert: only a test can tell the difference. To be entirely clear, if only a test can tell a cold and Omicron apart, then Omicron just is a cold.
The United Kingdom, with its record number of “cases,” most of which are surely false positives or extremely mild symptoms, promises to be a rehearsal for the US, so get ready for an Omicron “casedemic” here in the US — just like it’s unfolding now in the UK.
A recent CNBC story discusses UK data about Omicron symptoms, collected from a phone app over a wide number of “cases,” showing that Omicron symptoms are overwhelmingly mild and indistinguishable from the common cold. And then … the article warns the reader not to underestimate Omicron or to mistake it for a cold.
There is now a good amount of data about Omicron and its symptoms and hospitalization rates. UK and South Africa data show that it is extremely mild — basically a cold, and not even akin to a flu in terms of severity. A number of other studies now, as of late December 2021, support extremely mild symptoms and low hospitalization rates for Omicron cases, as reported by the New York Times.
Tim Spector, the UK scientist who developed the symptom tracking phone app used in the UK recently told the press:
Broadly what we’re seeing now is the majority of people testing PCR positive actually have cold-like symptoms and they do not have the classical triad of ill COVID symptoms of fever, loss of smell and taste and persistent cough. So it’s slowly emerged into a more symptomatic milder condition that looks just like a severe cold to many people.
It’s not just cases that are mild, it’s also fairly clear at this point that the large majority of hospitalizations allegedly because of Covid are in fact not related or are only minimally related to Covid. Omicron hospitalizations in South Africa have been overwhelmingly a product of testing for Covid upon entry into the hospital for any reason (i.e. no Covid symptoms were showing), as a report from the South African Medical Research Council’s Dr. Abudullah stated:
The majority of hospital admissions [66%] are for diagnoses unrelated to COVID-19. The SARS-CoV-2 positivity is an incidental finding in these patients and is largely driven by hospital policy requiring testing of all patients requiring admission to the hospital.
And yet despite all of the data overwhelmingly pointing toward Omicron being extremely mild and generally indistinguishable from a common cold, the linked CNBC article ends with this: “We’re concerned that people are dismissing omicron as mild,” he said. “Even if omicron does cause less severe disease the sheer number of cases will once again overwhelm health systems.”
Are we already in a “casedemic”?
“Overwhelming” health systems with Covid-19 cases, which are in the vast majority of instances false positives or mild symptoms, is the very definition of a “casedemic.” The “cases” warned about in the CNBC article are, based on the UK data cited, overwhelmingly asymptomatic or very mild cold-like symptoms. And it is these kinds of “cases” that threaten to overwhelm the system with unwarranted “cases” and “hospitalizations” and the consequent panic that our irresponsible media and political leaders are sowing through their ongoing mismanagement of pandemic responses.
It is quite obvious that what is happening in the UK now is a massive increase in testing due to panic about Omicron and a massive increase in false positives, which is inevitable when you ramp up asymptomatic testing with even accurate tests, let alone inherently flawed tests, which is what we do have (PCR and antigen tests are both extremely problematic for different reasons).
Harvard Medical School professor Westyn Branch-Elliman described in a US News & World Report essay how asymptomatic testing in school kids could lead to literally 71 out of 72 positive Covid test results being false positives. The same logic applies equally to all testing of asymptomatic people.
With testing of asymptomatic people becoming extremely widespread in the US and other countries, we are indeed seeing a tsunami of false positives. And with seasonal cold and flu making a comeback many people are now testing after showing cold or flu symptoms, and when the large numbers of Covid-19 false positives inevitably occur these people are tallied as confirmed “cases” for Covid-19, instead of the common cold or flu that they actually are.
And if we don’t get smart about these dynamics we may be stuck in an endless cycle of panic, increased testing, increased false positives, more panic, etc.
So what is the real impact of the pandemic?
In sum, Omicron at this point seems all much ado about nothing and continues the pattern of extreme exaggeration of all public Covid stats, following by the inevitable over-reaction from policymakers, politicians and the public that results.
I’ve personally been cautious in sharing my skepticism publicly. I’m a public policy lawyer who cares deeply about the common good and have made protecting the common good and the environment my life’s work.
But I am now, two years into this global nightmare, quite confident, based on a number of diverse lines of inquiry and data, that the pandemic is overwhelmingly a man-made and policy-made event, where it is the policy choices themselves that are causing the vast majority of harm, not the virus.
A good rule of thumb is to discount all public stats about Covid cases, hospitalizations and deaths by about 90% to get a more accurate figure of what’s actually going on. No, the US didn’t recently pass 800,000 deaths “from” Covid-19, as was widely reported. That figure is not remotely accurate because it includes all “deaths involving Covid-19,” as CDC describes clearly in its data, and this definition includes all people where Covid-19 is implicated in any way or is merely suspected of “contributing to,” as opposed to causing, the death. We must downgrade this figure by about 90% to get a more accurate figure of about 80,000 deaths over two years. This downward adjustment puts the Covid pandemic well within the range of seasonal flu deaths.
But the impacts from lockdowns, pseudo-lockdowns, and related policies have indeed been massive and will continue to be massive, unless people start to wake up and speak out about the absurdity of our pandemic policies at this point in time.
